
The Rosacea Guide

Rosacea is one of the most misunderstood conditions in skin health.
Most people get told they have “sensitive skin” and leave with a cream, an antibiotic, or a laser referral. Sometimes those things help. Sometimes they help a lot. But if you’ve dealt with rosacea for years, you already know the deeper truth: for many people, it keeps coming back because the skin was never the real starting point.
In my practice, when someone walks in with facial flushing, burning, visible capillaries, pustules, reactive skin, or eyes that constantly feel irritated, I am rarely thinking about the face first.
I’m already starting to connect the puzzle with:
mast cells & histamine
microbial overgrowth
oral microbiome
parasites
nervous system load
digestion
bile flow
inflammatory burden
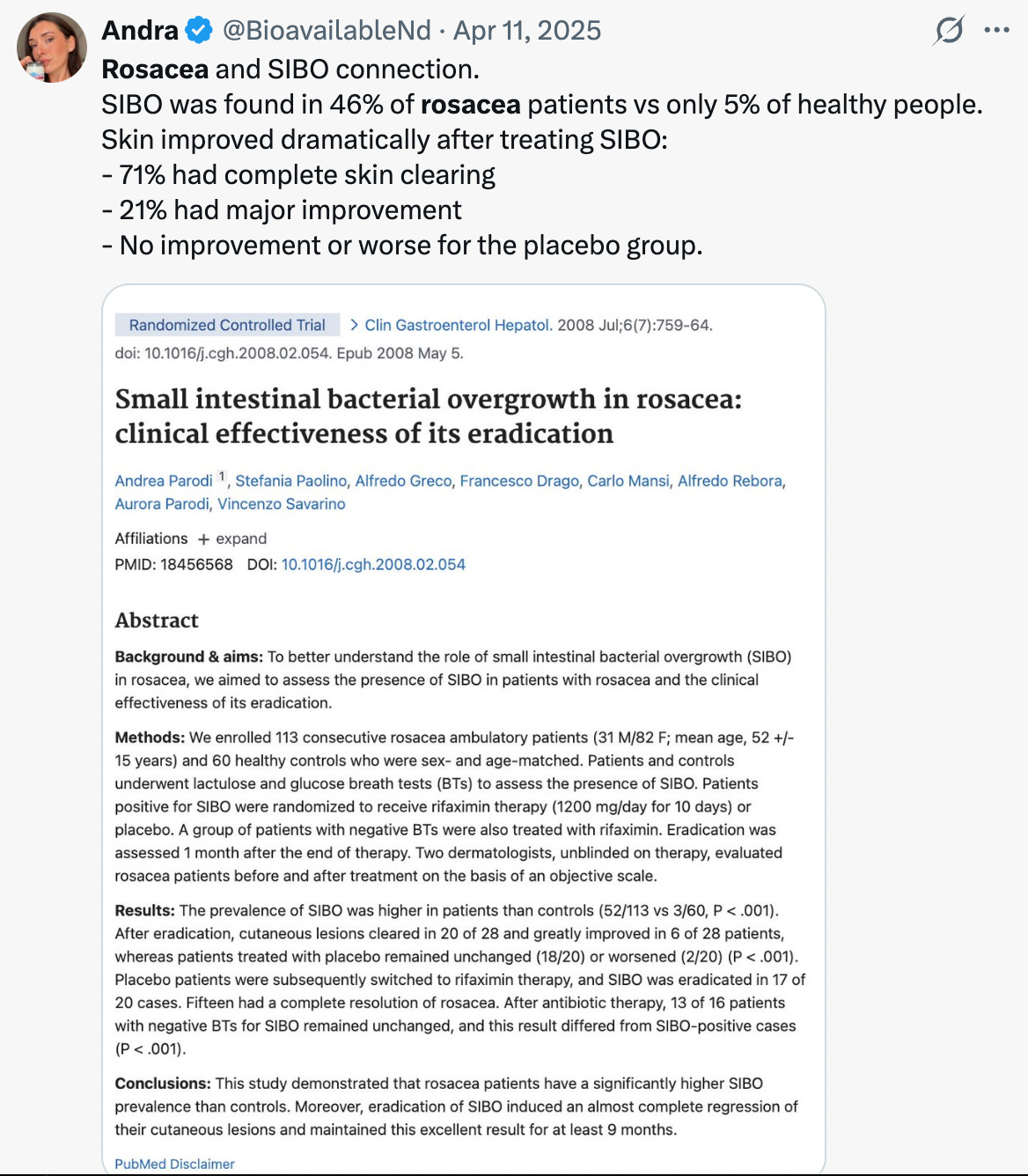
One of the most important rosacea studies ever published found that 46% of rosacea patients tested positive for SIBO compared to only 5% of healthy controls. After treating the SIBO, 71% had complete clearing of their skin lesions and another 21% had major improvement that lasted at least nine months.
That should completely change how we look at rosacea.
Root Cause Reasons
1. Small Intestinal Bacterial Overgrowth (SIBO)
This is one of the first places my brain goes in practice.
The small intestine is where nutrient absorption, immune modulation, microbial communication, and a huge amount of inflammatory regulation happen. When bacteria begin overgrowing where they should not, the immune system becomes more reactive, intestinal permeability rises, mast cells become easier to trigger, and inflammatory compounds begin circulating systemically.
The skin often becomes the overflow bucket.
These are usually the clients telling me:
“I bloat after everything.”
“My face gets red after meals.”
“I react to healthy foods.”
“I burp constantly.”
The 2008 SIBO study in rosacea is one of the strongest gut-skin papers we have in dermatology.
2. Parasites and Protozoal Terrain
This is the part of the conversation many people are uncomfortable having, but in my practice I see it far too often.
Not every rosacea patient has parasites. But in the right terrain, they absolutely matter.
Especially when the story includes:
travel history
constipation and diarrhea simultaneously
“I react to everything”
histamine issues
food sensitivities
back acne
A lot of chronic bacterial overgrowth patterns begin because something upstream disrupted the ecosystem first.
Parasites can impair:
secretory IgA
bile flow
gut motility
microbial balance
immune regulation
Once that terrain destabilizes, SIBO, histamine, mast cells, and rosacea often follow.
3. Mast Cell Activation
If you understand mast cells, you understand a huge portion of rosacea.
Mast cells sit at the intersection of:
nerves
blood vessels
skin
immune modulation
gut health
When activated, they release:
histamine
cytokines
inflammatory mediators
vasoactive compounds
Which means:
flushing
burning
swelling
redness
itching
heat
This is why so many rosacea patients flare with:
wine
heat
sunlight
stress
poor sleep
hard workouts
spicy foods
overheating
If your rosacea looks like this, I strongly recommend reading my MCAS Guide because it changes the entire framework.
4. Demodex Overgrowth
Everybody has Demodex mites.
The problem is when the terrain allows them to dominate.
The literature shows rosacea patients can have dramatically higher Demodex densities than controls. These mites may trigger immune activation through follicular irritation, bacterial proteins, TLR2 signaling, cathelicidin pathways, and mast cell cascades.
This is usually the patient with:
papules
pustules
rough “sandpaper” texture
itching
eyelid irritation
worsening at night
This is where topical ivermectin can become incredibly useful.
5. Oral Microbiome Dysfunction
This is one of the most underrated rosacea root causes.
The mouth is the beginning of the digestive tract, not a separate ecosystem.
If somebody has:
bleeding gums
bad breath
tongue coating
chronic sinus congestion
periodontal inflammation
mouth breathing
…that inflammatory burden does not stay in the mouth. Oral dysbiosis continuously feeds inflammatory signalling downstream into the gut and immune system. I see this pattern constantly in rosacea clients.
6. Low Stomach Acid and Digestive Insufficiency
Older dermatology literature actually found reduced pancreatic digestive function in subsets of rosacea patients.
That fascinated me because clinically it fits perfectly.
These are the patients who tell me:
“I feel heavy after eating.”
“Steak destroys me.”
“I can’t digest fats.”
“I burp constantly.”
Poor digestion creates fermentation. Fermentation creates dysbiosis. Dysbiosis creates inflammation. Again, the skin is usually downstream.
7. Leaky Gut and Secretory IgA Depletion
Once the gut barrier becomes more permeable, the immune system starts seeing things it was never supposed to see:
food antigens
endotoxins
microbial fragments
yeast byproducts
Now combine that with low secretory IgA and you get a terrain that struggles to regulate microbes while simultaneously overreacting to normal inputs.
This is where you start seeing:
food sensitivities
histamine issues
bloating
eczema overlap
reactive skin after meals
8. Nervous System Overload
Some rosacea cases are heavily nervous-system driven.
The patient is overstimulated, overtrained, underslept, stressed, highly driven, constantly “on,” and running on cortisol and caffeine.
The body loses resilience.
Mast cells become easier to activate. Blood vessels dilate more easily. Thresholds become lower.
Then suddenly:
a hot shower
a hard workout
a stressful conversation
a glass of wine
…is enough to light up the entire face.
Andra’s Recommendations
Before getting into my recommendations, I want to make one thing very clear. Rosacea clients often live in a body that has lost a lot of resilience. The nervous system is maxed out. The gut is sensitive. Mast cells are firing “randomly". Sleep is poor. Recovery is even poorer. The body starts reacting to normal inputs like they are threats.
